Does anyone have a departmental policy of what to do in the case of a high TVC/Endo count?
The standard reply is to continue but without HDF, but why?
As we know when you get your high result you have already done a week on water that wasn't up to spec.
Usual response is to retest in case of handling/lab error so that's another week on HD rather than HDF
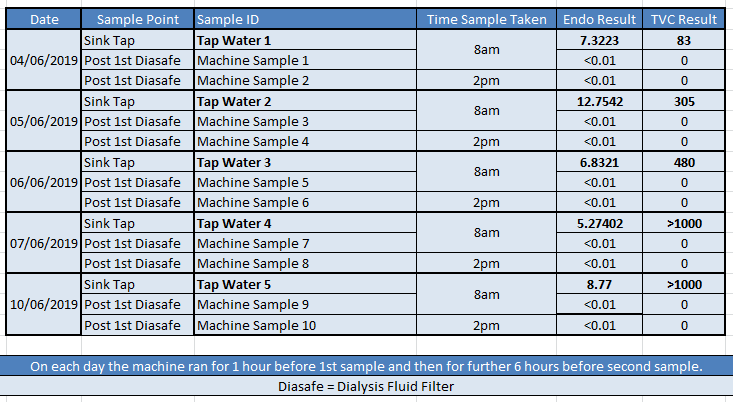
I'm thinking of doing an experiment; running a machine on tap water (to enable a consistently high TVC/Endo count) in the workshop and sampling both the raw water and the HDF sub fluid on a daily basis for a week to see what happens.
I personally think the endotoxin filters can handle it...
Anyone else done similar or have any thoughts?
Will technology prevail over what people MAY think happen??
Ian Wilde